
Cape Fear Valley’s Cumberland County EMS Protects Staff from Career Shortening Injuries

Cape Fear Valley Health System Mobile Integrated Health is based in Fayetteville, North Carolina and has a mission to provide exceptional healthcare for all their patients. But Cape Fear Valley does much more than that; their commitment to looking after their 165 paramedics and EMTs is remarkable.
After taking up the position of Chief at Cape Fear Valley’s, Cumberland County EMS, David Grovdahl, an experienced EMS professional, worked quickly to assess the health of his team. His key objective was to build a well-equipped and prepared staff, but with the service recording 4-8 musculoskeletal injuries every month it became clear very quickly action was required to improve safety for the staff.
Injury related lost time was costing the Service on average $18,000 per injury, with annual costs escalating to in excess of $300K. In addition, with so many workers off injured at any one time, it meant that there were occasions when the service could not put all their trucks on the road.
The situation was not a surprise to Chief Grovdahl, who had encountered a similar position in his previous role with a governmental based EMS system. Here, after researching the best assistive equipment to support workers when moving and handling patients, he placed lifting cushions on ambulances and reduced injury rates by 50%.
In the Fall of 2021, Chief Grovdahl made the decision to put ELKs (Emergency Lifting Cushions) on the four quick response vehicles at Cape Fear Valley. ELKs can be utilized for fallers weighing up to 1,000 lbs. and the vehicles became the first choice when responding to lift assist calls. If an ambulance is deployed to a lift assist situation but an ELK is the better solution for both the patient and EMT or Paramedic, the protocol has become that they call for support from the quick response team.
In the last couple of months Chief Grovdahl has already seen injury rates reduce to just 2 a month, a significant improvement on previous rates.
Chief Grovdahl says, “When I started out working in EMS 22 years ago, I was told I would be lucky to survive 5 years without picking up a career shortening back injury.
“I’ve always been particularly careful to protect my physical health and we’ve seen some great improvements in lifting techniques in that time, but using assistive equipment is vital for the long-term health and wellbeing of our Paramedics and EMT’s.
“EMS is a rewarding career but professionalizing the way we work for the greater good of our patients and staff must be a priority if we are to attract the best people into the industry.”
The use of assistive lifting devices can reduce the risk of back injury among health care workers (D’Arcy et al., 2012; Andersen et al., 2014) and Chief Grovdahl’s team at Cape Fear Valley are seeing this for themselves firsthand.
When the Inflatable Lifts Replace Bended Backs

Introduction
This project takes as its starting point the fact that approx. 1,700 times every year, an elderly citizen in the City of Copenhagen falls in their home and cannot get up again without help. Employees in home care are called out to these falls, but it is often also necessary to summon assistance from the fire brigade.
This has meant that citizens have often had to lie on the floor for more than 1 hour before help arrives, as the fire brigade’s main tasks are emergency, life-threatening events.
A pilot project looked at opportunities for new technological solutions to the problem and discovered new possibilities to rethink the task so that the use of the fire brigade could be reduced and thereby also the waiting time for both citizens and employees.
This resulted in two mobile lifts being tested in two home care units in 2008. The pilot project showed that the changed work routines that resulted from the introduction of the new tool, not only provided a better but also a more effective solution to the task and a better working environment for the employees.
Helping up older people who have fallen
The background for a project that focuses on developing and testing the equipment is that it is typically moving the position from lying to sitting that is most difficult for the citizen, and which represents the major occupational strain for the carer, as this involves ‘dead weight’ when citizens cannot do anything themselves to help.
It must first be emphasised that the circumstances of each case are always unique. But there are two characteristic working procedures:
- A citizen calls on their emergency alarm when they have fallen and cannot get up. The Homecare Service sends out two employees, one of whom is from the nursing group.
- A carer comes on a scheduled visit to a citizen and discovers that they have fallen. If the carer cannot guide the citizen, they call the Homecare Service and summon assistance. If the carer is in the slightest doubt about whether the citizen has been injured, the assistance shall be provided by a nurse.
Due to the potential occupational strain from lifting a citizen up from the floor, the working environment instructions are that the employees must initially try to guide the citizen up so that the citizen can get from the floor to a chair or bed by their own efforts. In those situations where the employees cannot guide the citizen up, the City of Copenhagen has an agreement with the fire brigade that they will be called for assistance.
Project goal and labour-saving potential
The goal of the project was to optimise the working procedures of the Homecare Service by introducing mobile lifts as permanent aids.
Before the start of the project, the Homecare Service used an average of 150 minutes on the falls where employees could not guide the citizen up and had to summon assistance from the fire brigade. It was expected that by having mobile lifts available, the Homecare Service would be able to solve the same kind of falls in 2 x 25 minutes with two employees (50 minutes in total).
Since there are 1,700 falls every year, where the employee cannot guide the citizen up, the anticipated time-saving potential in the City of Copenhagen was approximately 5.2 FTEs or DKK 1.6 million annually.
The project was also expected to have a number of positive side-effects, such as an improved working environment and improved citizen services. This is because the introduction of the mobile lifts would entail a more gentle lifting procedure for both the citizen and the employee.
Success criteria
The project is designed around the achievement of the seven criteria for success:
1. The labour-saving potential.
By introducing the technology of mobile lifts, there is a proven savings potential for homecare in the City of Copenhagen of approx. 5.2 FTEs or DKK 1.6 million annually.
2. More falls can be handled without using the fire brigade
There is an increase in the number of fall situations that the home care service can handle without using the fire brigade.
3. The employees’ perspective
The employee experiences a more caring handling of the task “Up from the floor after a fall” through the use of the mobile lift technology. The employees experience a labour-saving potential as positive.
4. The citizens’ perspective
The citizen experiences a more caring handling of the task “Up from the floor after a fall” through the use of the mobile lift technology.
5. The organization
There is a successful organisation in relation to storage, transportation and maintenance of the mobile lift technology.
6. The training
The relevant home care employee completes a training course in the use of the mobile lift technology in the form of an introductory course, on-the-job training and a general introduction to techniques for moving people.
Technology
The pilot project had demonstrated that the employees were open to the use of a mobile lift and to solve the task themselves. But it also became clear that it was very important that the mobile lift was reliable. If the employees felt that they could not rely on the lift, they chose not to use it from the outset.
Based on a number of qualitative and quantitative requirements, it was decided to purchase mobile lifts of type Mangar ELK.
The ELK is an inflatable lifting cushion that allows two employees to lift a citizen of up to 450 kg from the floor without straining the employees’ backs. The seat height of 56.5 cm means that when the cushion is inflated, the citizen can get up by themselves (or with support from the employees) and stand by their walking frame, sit in a chair or on a bed.
The ELK weighs a total of 9.7 kg and consists of a 5-compartment lifting cushion, a compressor and a hand control. The four cushions are filled with air from a small portable compressor. As the compartments fill with air, the citizen is lifted up until they are at a height where the employee can move them without straining their back.
The pilot project had shown that the most suitable solution was to place the mobile lifts in the Homecare Services nursing cars. Since a qualified nurse’s assessment is required in fall cases, this ensures that the lifts can be quickly deployed at the citizen who requires assistance to get up off the floor after a fall. It was considered that the requirement would be covered if each homecare unit was equipped with 3 mobile lifts each.
Data basis
The evaluation was conducted by Arbejdsmiljø København [Working Environment Copenhagen] and provided an overall impression of the impact of the introduction of the mobile lift on homecare.
The evaluation is based on qualitative and quantitative data collected from six different sources:
- An evaluation workshop
- Participant observation
- A limited registration of the use of mobile lifts
- Collected data on the use of the Copenhagen Fire Brigade.
- Analysis of selected parts of the City of Copenhagen’s satisfaction measurement
- Interview with the 2 instructors from Arbejdsmiljø København
Results
Success criterion 1: The labour-saving potential.
By introducing the technology of mobile lifts, there is a proven savings potential for home care in Copenhagen Municipality of approx. 5.2 FTEs or DKK 1.6 million annually.
It was expected that by having mobile lifts available, the homecare service would be able to solve the same kind of falls in 2 x 25 minutes with two employees. It takes two employees to help a citizen up from the floor with a mobile lift after a fall. The evaluation showed that on average, 2 x 22 minutes were used by two employees.
The recording of falls in the two home care units and in the 24-hour service (Døgnbasen) showed that the total time used by the two employees ranged from 10 to 80 minutes. The large variation may be explained by the fact that there are major differences between the extent to which the citizens can cooperate, and how long it, therefore, takes to get the citizen standing by their walking frame, sitting in a chair or lying on a bed.
The baseline measurement showed that before the start of the project, the homecare service used an average of 150 minutes on the falls where the employee could not guide the citizen up and needed to call for assistance from the Fire Brigade.
Since there are 1,700 falls every year, where the employee cannot guide the citizen up, the time-saving potential in the City of Copenhagen was approximately 5.6 FTEs or DKK 1.85 million annually. ((method: 1,700 falls x 106 minutes/940 hours average annual citizen time per employee (average for social and healthcare worker and nurse)) x (1940 gross annual norm per. employee/940 hours) x (DKK 170 average hourly wage from fldnet.dk) – (1 FTE for practical organisation)).
Success criterion 2: More falls can be handled without using the fire brigade
There is an increase in the number of fall situations that the home care service can handle.
The Homecare Service entered into a new cooperation agreement with the Copenhagen Fire Brigade in July 2009. The purpose of the agreement is that the Homecare Service shall have the necessary assistance from the Copenhagen Fire Brigade in connection with citizens who have fallen in their own homes.
The service is limited to cases where the citizen has fallen in their own home and where the Homecare Service cannot help them to their feet again. Even when the Fire Brigade has arrived, the homecare service is responsible for the citizen and cannot leave the citizen, even after the Fire Brigade has arrived.
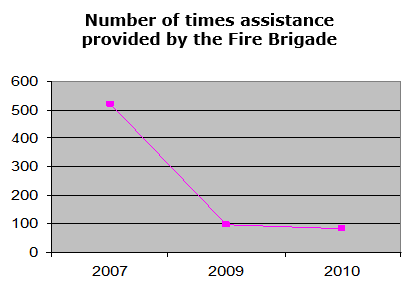
In 2007, the Copenhagen Fire Brigade was called to assist in 520 cases of falls in citizens’ own homes. This dropped to 96 trips in 2009 and an estimated 84 trips in 2010. The registration survey showed that in only 4% of the falls where the mobile lift was used was it necessary to give up and call for assistance from the Fire Brigade.
The reason that there was a significant decline already in 2009 is that there was confusion in relation to a new agreement from September 2009. Here, a number of employees had mistakenly believed that they could not summon the Fire Brigade, but should deal with all falls themselves.
The figures for 2011 onwards are likely to be even lower in step with the mobile lifts being fully integrated into the daily routine and especially when there is a satisfactory solution to the problem that the mobile lifts are viewed as heavy and awkward to transport.
Assuming that the number of falls requiring assistance remains constant, a decrease from 520 trips in 2007 to an estimated 84 trips in 2010 indicates that assistance from the Fire Brigade was only required in 16% of the cases. Since the target was 15 %, it must be concluded that the project has achieved its goal.
Less psychologically stressful cooperation
The evaluation shows that the Homecare Service’s increased opportunities to help a citizen up after a fall is perceived as an improvement of the psychological working environment.
There have previously been many cases where employees felt that the firemen who were summoned, questioned whether there really was a need for assistance. This was perceived as psychologically stressful, which reinforced the feeling of helplessness that many employees experienced when they had been forced to let a citizen lie on the floor for a longer period because they could not guide them up.
“One of the best things has been that we no longer have to deal with angry firemen” (Employee in the Homecare Service)
“We do not have to deal with the same conflicts when we call the Fire Brigade now, because we can say that we tried ourselves” (Employee in the Homecare Service)
Success criterion 3: The employees’ perspective
The employee experiences a more caring handling of the task “Up from the floor after a fall” through the use of the mobile lift technology. The employees experience a labour-saving potential as positive.
For the employees, the labour-saving potential was only of minor importance for their positive perception of the mobile lifts.
The time aspect has a more concrete and practical significance for the employees. Firstly, time plays a role in relation to named irritation over the long waiting time for assistance from the Fire Brigade. Secondly, it is significant because it is in the nature of things that it is impossible to predict when a fall will occur, and it is an urgent task. There is a major risk, therefore, that the longer the task takes, the more it will interfere with the other tasks in a busy schedule and this increase stress levels.
“The ELK results in fewer changes to the schedules. (Group Leader)
For the employees, however, it very important that the mobile lifts are aids that facilitate their work in relation to a very specific and difficult task. They experience the mobile lifts as a useful tool.
“It is quite difficult to understand that we have not always had it. It is a natural part of the work.” (Employee)
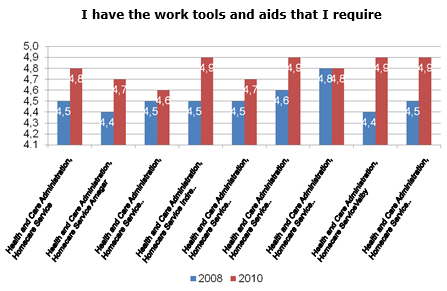
If we consider one specific question in the City of Copenhagen’s job satisfaction surveys from 2008 and 2010 respectively, “I have the tools and resources I need”, we see a clear, positive development in all the home care units. The increase is between 0.1 and 0.5 percentage points.
It is experienced as very positive that the employees have new options in terms of helping an individual who has fallen.
“We are very pleased with the ELK and so are the citizens. They can get up without any pain and stand up spontaneously from the ELK” (Employee)
The employees explained that it is of major importance to them that they can do the job themselves: That they can help the citizen all the way up, make sure that the citizen is well and then move on to other tasks – instead of having to sit and wait for up to one hour for assistance. It gives them a sense of authority and competence in performing their tasks.
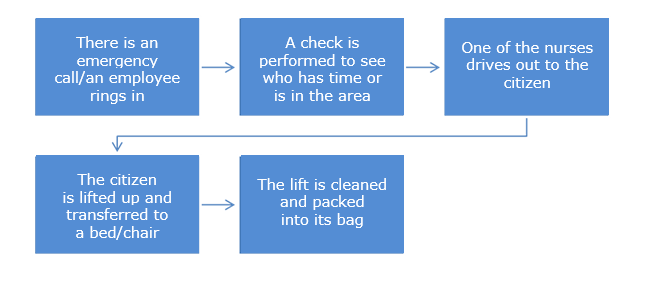
It requires a certain amount of practice and good cooperation between the two employees to lift a citizen successfully with a mobile lift. One employee prepares the cushion and the compressor, while the other talks to the citizen, explains what will happen and ensures that there is a chair or a walking frame ready for the citizen to use.
Together, the two employees get the citizen onto the cushion, possibly by using a slide sheet. One employee operates the mobile lift, while the other stands behind and supports the citizen. When the citizen is up and placed in a chair or bed, the mobile lift is cleaned with spirit and packed into the bag.
Proper use of the mobile lifts requires that the employees can communicate with the citizen. It is difficult if the citizen is very confused, intoxicated or otherwise unable to cooperate. This can sometimes mean that the task must be abandoned and the Fire Brigade is called.
The only recurring criticism in relation to the use of the mobile lifts is that it is perceived as heavy and awkward, especially when it has to be transported up to e.g. the fifth floor. For some employees, the difficulty of transporting the mobile lift became an excuse for not accepting the new tool.
“I’m not so big, and I think it is difficult to carry. So I must admit that I don’t take it up with me often enough if, for example, it is a fifth floor apartment and I know that the staircase is narrow” (Employee)
The producer is developing a prototype in a backpack as a solution to the transport problem. This has occurred through input from e.g. the Homecare Service.
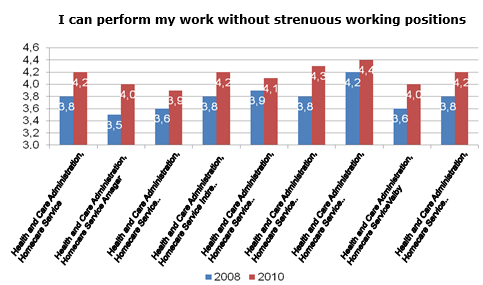
The evaluation shows very clearly that employees have experienced that the implementation of mobile lifts as a work tool has reduced both the physical and the psychological working environment impacts associated with helping a citizen up from the floor after a fall.
“The back pains are not as bad as before. You could get really tired after a long night.” (Employee)
The physical strains occur when the employees try to move the citizen off the floor. Transfer from the floor represents a particular strain on the body because it is impossible to keep the spine in its natural, neutral position or to avoid twisting and bending the back during the transfer.
The psychological stress arises partly as a result of the stress and helplessness experienced as a result of being unable to help a citizen out of an unpleasant and undignified situation and having to wait a long time for assistance from the Fire Brigade. But stress also occurs when other scheduled tasks have to be postponed at short notice in order to deal with an emergency situation.
In addition to the mobile lifts reducing the actual occupational work load, it also affects the working environment in a more indirect way, by focusing on the potential stress inherent in transfer tasks. This occurs because the use of an aid like a mobile lift helps to make employees aware that it is a transfer task that strains the body.
“There is a greater understanding among the employees of the importance of transfers and prevention” (Working environment manager)
However, one should be aware that the use of a mobile lift may in itself cause strain on the body because the employee must transfer the citizen from the floor onto the cushion of the mobile lift.
“This can be difficult because one has to kneel down and take hold of the citizen who is on the floor” (Employee)
In addition, some employees find it a burden having to transport the mobile lift up the stairs:
“Nurses have a sore lower back after carrying the ELK from the car, along the street, and up to the third floor and by standing in an inappropriate position while the device is operated.” (Working environment representative)
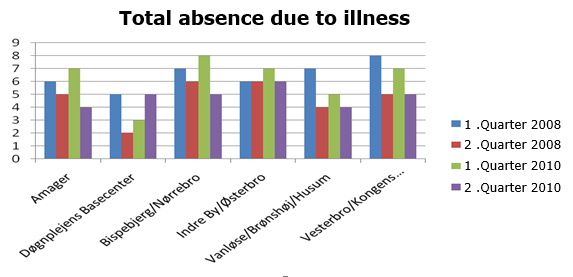
It is generally believed that the use of mobile lifts has had a positive effect on the number of occupational injuries. It has not been possible to see whether this is reflected in the reported injuries.
It is generally believed that the use of mobile lifts has had a positive effect on the number of absences due to illness. However, it has not been possible to see whether this is reflected in the statistics compared with the first two-quarters of 2008 and 2010 respectively.
Success criterion 4: The citizens’ perspective
The citizen experiences a more caring handling of the task “Up from the floor after a fall” through the use of the mobile lift technology.
The citizen is made to feel safe by the fact that the employees can reassure the citizen, tell them what is going to happen and support the citizen during the lifting. It is also of great importance that the citizen can quickly get out of a situation that is uncomfortable and undignified.
“People had a pleasant “up from the floor” experience – it is very calm” (Employee)
Some citizens experience the situation of using a mobile lift as cumbersome and slow because, after all, it takes time to deploy the mobile lift and pump up the four cushions. They have difficulty understanding why the employees do not just lift them up. However, this is an issue that was even clearer when they had to wait for the Fire Brigade.
“Some say – can you not just take hold here and help me up?…” (Employee)
It requires a certain degree of cooperation by the citizen to use the mobile lift. The citizen must be able to communicate with the employee and must have some ability to balance so that they can sit on the cushion during lifting. This means that if the citizen is very confused or intoxicated, the employee must give up and call the Fire Brigade.
This problem could be solved by the Homecare Service supplementing the model of mobile lift used in this project with a larger model that also has a back and armrests. It should be noted here, however, that this would probably be somewhat heavier than the mobile lift used in this project.
“She was very drunk and it was difficult to determine how much she understood. It would probably not have worked if we two had not known each other well” (Employee)
It has not proved useful to prepare the planned information material for citizens about the technology and about the citizen’s role in the use of mobile lifts. The fall situations are often experienced as being unique, where it is the direct communication between the citizen and the employee that is decisive.
“The citizen was very pleased with the ELK, even though it was a new experience for them” (Employee)
Sometimes, the situation involves citizens who would have very little benefit from written information. However, one can imagine that if the idea was implemented to place a mobile lift permanently in a home where the citizen falls frequently, it would be appropriate to provide more formal information.
Success criterion 5: The organisation
There is a successful organisation in relation to storage, transportation and maintenance of the mobile lift technology.
The organisation and administration of the mobile lifts have quickly become an integral part of each home care unit’s daily operations and therefore also reflect the differences that exist between the organisation of the various units.
In some units, all three mobile lifts are placed in the nursing cars, while in others only two lifts are placed in cars, while the third is stored with the nursing manager. Placing the lifts in the cars is due to the fact that in the City of Copenhagen, it is the normal practice that a nurse will be summoned in case of a fall. The nurse uses a car as the means of transport, since there may be long distances between those who receive nursing care. The mobile lifts are therefore stored in the car permanently.
Because the homecare units have more than three cars each, some coordination is also required. However, the evaluation shows that this does not cause problems.
“The others know that I have the ELK in the car. So they cover for me when I need to deal with a fall in their area” (Employee)
A generalised outline of the working routine could look like this:
It was estimated in the project application that a total of one FTE would be used in the entire Homecare Service for the administration of the mobile lifts. It has not been possible to record the specific amount of time spent on the administration of the mobile lifts because, in step with the implementation, it has become an inseparable part of the general administrative work around the use and maintenance of aids. But the evaluation discovered no expressions of irritation that the implementation of the mobile lifts was an additional administrative burden on the homecare units.
The small amount of time spent on administration was also thanks to the fact that the ELK was very reliable (unlike the mobile lift used in the pilot project) and it was therefore only necessary to contact the manufacturer on a few occasions.
“There is very rarely anything wrong. But otherwise, the way it works is that those who have used the ELK are also responsible for reporting back if there are any problems” (Team leader)
Success criterion 6: The training
The relevant homecare employee has completed a training course in the use of the mobile lift technology in the form of an introductory course, on-the-job training and a general introduction to techniques for moving people.
Good instruction in the use of a new aid minimises the risk that the employees shied away from using a mobile lift, either because they did not feel competent or because they did not appreciate its potential.
The specific target group for the courses was mainly the resource persons for transfer in the Homecare Service and the 24-hour service who perform the task in relation to falls and who are in direct contact with the citizens in case of a fall. The knowledge they acquired about using the mobile lifts could be used both in their own work and for the instruction tasks they have in the individual homecare units.
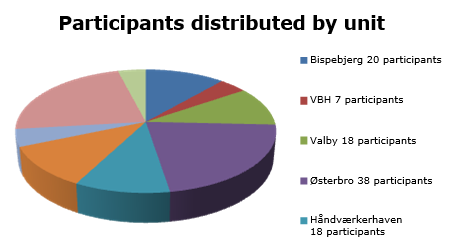
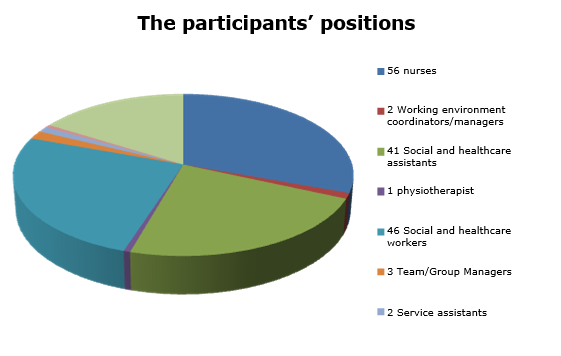
A total of 178 employees participated in one of the 9 courses. All the homecare units participated, but with very different numbers of employees. This was primarily due to the different ways of organising the training locally. The employees were divided between all the different professional groups:
The course lasted 3 hours and was conducted in Arbejdsmiljø København’s “bed ward”.
The teaching was divided between practical training in the use of mobile lifts and more general training in transfer techniques.
The practical training was designed to instruct personnel in the use of the equipment. The course participants were familiarised with the mobile lift and they worked with it so they became comfortable using it. At the same time, they had an opportunity to give their immediate reaction to the mobile lifts and could suggest improvements. Those who had used a mobile lift in practice were able to talk about their experiences.
“It’s very effective when some of the course participants can tell the others that it is a good tool” (Instructor)
When the employees are comfortable with the use of the lift, there is less risk that they return to lifting the citizen or calling the fire brigade unnecessarily. Finally, the employees’ confidence reassures the citizen, so they are not “afraid” of the new, unfamiliar methods.
The overall training in transfer techniques provided the course participants with knowledge about transfers at floor level. They have learned about working posture and methods to avoid the most stressful postures and movements.
“It is very important that the employees receive structured instruction in the use of a mobile lift and get an opportunity to try it. Otherwise, there is a risk that it will end up unused in a corner.” (Instructor)
The employees experienced the training as very meaningful and fruitful. They have subsequently been able to train their colleagues at local, joint weekly group meetings so that they all became qualified to operate the mobile lifts.
The instructor’s assessment is that the training could have been cut down to two hours, without affecting the quality.
Success criterion 7: The technology
The project used a tender process to ensure the best private partner in relation to the economy, quality, technology development possibilities, service, etc.
The tender process was completed without any problems. Based on lessons learned from the pilot project, it was possible to establish clear technical and qualitative requirements for the lifts and to select the most qualified product called the ELK.
The tender documents emphasised that the mobile lift should be able to perform the task ‘up from the floor after a fall’ by lifting a person from the floor level to a height of at least 55 cm.
It also included a number of requirements based on the needs of the employees:
- Low lift of total weight (maximum 5 kg/10 kg.)
- Low total weight (maximum 10 kg.)
- It should be easy to clean the lift
- It should be easy to transport the lift (even climbing stairs)
- It should be easy to instruct new users in the use of the lift.
Finally, two requirements were based on the needs of the citizen:
- High user weight (minimum of 250 kg.)
- The citizen should feel safe while being lifted.
There were two suppliers who submitted offers, but only one could meet the requirements. A contract was concluded with that supplier. The contract has no set term but runs initially for one year and the lifts are then expected to be included in the general municipal operations.
Summary
The project fully met its goal. It has proved possible to optimise the working routines by the Homecare Service’s employees themselves using mobile lifts to help citizens up off the floor after a fall, instead of having to wait for assistance from the Fire Brigade.
The optimised working routine is estimated to free up labour corresponding to 5.6 FTEs. This is 0.4 FTEs more than the estimated labour-saving potential.
Before the start of the project, the Homecare Service used an average of 150 minutes on the falls where employees could not guide the citizen up and therefore had to summon assistance from the Fire Brigade. It was expected that by having mobile lifts available, the Homecare Service would be able to solve the same kind of falls in 2 x 25 minutes with two employees. The evaluation showed that on average, 2 x 22 minutes were used by two employees.
The project included a 3-hour course conducted by Arbejdsmiljø København for the resource persons in transfer in the home care unit and the 24-hour service that performs the task in relation to falls. These people subsequently trained their colleagues. A total of 178 employees, distributed between all the home care units and the 24-hour service, participated in one of the 9 training sessions.
Doctor Explains The Importance Of Post Falls Assessment Tool, ISTUMBLE

“The reason I became involved with the ISTUMBLE project is that it is so profoundly positive for residents of care homes and those who care for them.
The benefits of lifting a resident off the floor are innumerable. By definition residents of care homes are frail – otherwise, they would not be cared for in a residential context. With frailty comes a lack of physiological reserve and strength. In addition, residents may have multiple co-morbidities involving the major body organs – respiratory/ lung disease, cardiovascular/ heart and vessel disease and renal disease/ impaired kidney function. All these co-morbidities cause reduced skin perfusion. Thus when a resident is kept on the floor for more than 20 minutes the pressure from the floor, especially on bony prominences of the body, further reduces blood supply to the skin. Therefore an elderly person on a hard floor or even a carpet will suffer an early breakdown of skin tissues and ulcer development. The most common complications of skin ulcers are increased mortality, osteomyelitis, and sepsis. If the patient has sustained a femur fracture during the fall the chances of mortality from the pressure ulcer are higher still because the patient will suffer reduced mobility both before and after surgery.
In 20 years of emergency medicine, I have never seen an exacerbation of damage to a broken femur of an elderly patient who has been carefully lifted with an appropriate lifting device.
Other than in the exceptionally unlikely possibility of a neck injury – not lifting the patient who has fallen as a result of any cause I believe is both unacceptable and unkind. As an aside I have never seen a resident of a care home sustain a fracture of neck vertebrae after a fall. I have only seen this from falls of elderly people falling in the street (concrete usually involved).
Of course, should a patient be in cardiac arrest they should not be lifted.
GP’s will not attend patients who are on the floor. Once lifted the GP can visit and thus prevent many trips into busy, loud and excessively lit Emergency departments. Such places are frightening for frail and demented people. Not sending the patient means that care staff is not obliged to travel with the resident preventing attrition of care staff who are needed at the care home.
Finally lifting patients from floors allows carers to continue to do just that – care. Carers become immensely upset to see their residents wait hour after hour on the floor because hard-pressed ambulance services cannot attend. When I have delivered this teaching to care homes there has been overwhelming relief felt by empowered care staff, empowered by education and ability to act.
– Dr Sue West-Jones, a consultant in Emergency Medicine
If you would like to download the free post falls assessment tool, please visit the Apple Store or Google Play Store and search for ‘ISTUMBLE’.
To access the “IStumble” App in the Apple Store CLICK HERE
To access the “IStumble” App in the Google play Store CLICK HERE
Veteran Talks About How PTs and OTs Helped Him Overcome His Circumstances

Darren Swift lost both his legs and sustained other injuries when he was blown up by a homemade grenade, consisting of a coffee jar, Semtex and shipyard confetti (nuts, bolts, screws).
Darren, also known as Swifty to his friends, spent the next 18 months going through rehabilitation trying to come to terms with his new way of life; the life he had nearly lost.

Darren explains; “When I was in hospital and all bandaged up, I was assigned a PTs, Alison. She was my PT and sort of stuck to me like glue, really.”
“Every morning I was in the gym or the hydro pool doing some sort of exercise with her. It was good because it was that which kept me moving, both physically and mentally. It’s good to have a focus and keep your brain occupied when you’re trying to cope and come to terms with what has happened.”
Darren continues, “Alison’s work method was patient-led. She’d explain to me what activities and exercises we should be doing at the point in the rehabilitation, followed by the question of how much of it I’d thought I could do and then we’d have a go at it.
For example, I remember I couldn’t swim, it really messed with my head especially as I was a good swimmer when I was able-bodied.
I remember when I first jumped in the pool to do some exercises with Alison, I sank to the bottom and I just about made it to the side.
I was beside myself. I couldn’t believe I’d lost my ability to swim. I mean, I really couldn’t swim.
There was nothing I could do to make myself stay on the surface and no matter how much I waved my arms around I could not swim. This lasted for around four months.
Darren’s sense of humour comes across when he talks about; “I would call myself the Michelin man because before I got in the pool, I’d have rubber rings and buoyancy aids strapped to every part of my body and I basically just bobbed about in the pool.”
I looked ridiculous I really did, it looked very comical I wished we had taken a couple of photos back then, but this was before the days of cell phones.”
Darren’s determination and resilience pushed him to continue to try and learn to swim again.
“Anyway, we persevered, or she persevered with me. I was getting more and more frustrated because I knew I could swim but I’d just forgotten how, and I couldn’t do it.
You get absolutely no propulsion at all when you just have stumps, no propulsion at all. No matter what you do with them you’re not going to drive yourself forwards or backwards or anywhere; so it’s all about your arms.
One day I’d had a bad night’s sleep and I wasn’t feeling brilliant. As I got to the pool Alison said ‘Come on lets get all these rubber rings on you’ and I said no not today.”
I sat down on the side of the pool and took a deep breath and sort of launched myself into the pool and I came up swimming. I just bobbed to the surface and started swimming and it was just bizarre. It just came back to me, I just started swimming.”
Darren went through rehabilitation for 18 months in which he had encounters with PTs and Occupational Therapists and has many more positive stories regarding his experiences with them.
“OTs helped me learn how to be independent again. I’d have cooking lessons and be taught how to use computers and see how well the dexterity was in my hands, after losing some of my fingers.”
Darren continues to be independent to this day and travels around the world snowboarding, parachuting and giving back to the community that had helped him through charity work; something which he is very passionate about.
Southfield Fire Department, Michigan

Southfield Fire Department serves the 175,000 citizens of Southfield and Lathrup Village, which includes a large elderly community. The department has 88 staff members and 5 fires stations located across the region.
In 2014, the busiest year on record, firefighters responded to 13,470 calls for service (36.7calls per day), and remain the busiest fire department in Oakland County.
Southfield Fire Department has used Mangar lifting cushions, ELK and Camel for more than 14 years. An early adopter of the products, the service has 12 lifting cushions which are used regularly every week to lift fallen patients.
Captain Melissa Medici explains, “The lifting cushions are ideal when we need to assist a citizen who has fallen in a confined space, whether at home or in a public space. We have a large elderly population in our district and falls are common.
“They are also great for lifting heavier, obese patients. Increasingly patients are weighing in over 300lbs and the cushions help us move the citizen safely, particularly in situations where we can’t get other equipment into a room. This means we can ensure there are no delays to patient care”.
Southfield Fire Department also value the health and wellbeing of their work force and report the lifting cushions save the backs of the EMTs and paramedics. Captain Medici is very aware of the very high work related injury rate to EMS workers nationally in the US and is keen to protect her own employees. She says, “Having used the lifting cushions for many years, we have seen a reduction in back injuries to our work force. We see that as a considerable benefit to using the equipment”.
Case Study: EMS Chief Blames Chronic Back Pain On Lifting Practices

Daniel McGuire was a field EMT for 23 years before chronic back problems brought the EMS career he loved to an abrupt end. After two painful failed back operations, doctors ruled out Daniel ever returning to the EMS work he’d enjoyed since high school and the sense of, ‘giving back to his community’.
Daniel started volunteering with Geneseo Fire Department, New York in 1978 and soon found himself looking forward to his next shift and the camaraderie shared with colleagues. His colleagues became his second family; eating together, looking after each other and sharing many experiences – both good and bad.
Daniel’s early days
In the early days of his EMS career, there was no equipment to help lift patients and a gurney that weighed 65lbs. empty. Patients needed to be physically lifted by a minimum of two EMTs, who often had to twist uncomfortably to place a stretcher in an ambulance. The regularity of the lifting and twisting placed incredible stress on the lumber area of the spine and hips, causing most EMTs to complain of aching backs. At the time they felt unable to say anything to superiors for fear of ‘losing face’. They felt if it was revealed they had an injury, others may think they weren’t up to the job.
In 1987 Daniel moved to Henrietta Volunteer Ambulance; a much larger agency with over 5,000 call outs a year. As well as his volunteer work he was a Sales Representative at Eastman Kodak, but much preferred his life now as an EMT- Intermediate. By now, the pain in his back and knees was becoming unbearable and increasingly difficult to manage. He used ice, heat and medication to manage the pain but continued to put patients first – whatever they weighed – and the trauma to his back continued to worsen.
Eventually, surgery was the only solution. After two operations on his spine, Daniel was told his back was too fragile to return to the job he loved and he would never work in the field again. He returned to administrative duties but began to sink into a depressed mood, terribly missing the active EMS field work. He started to notice how the physical and demonstrative stress of the work affected other EMTs and paramedics. The physical pain was only surpassed by emotional pain and marriage breakdowns, chemical dependency and suicides were beginning to rise among the ranks.
After Kodak folded 15 years ago, Daniel started to work for himself and founded CISM Perspectives, Inc. (www.cismperspectives.com) in Rochester, New York. His aim is for EMS, Fire and Law Enforcement agencies to make the wellbeing of the EMT the priority and to gain recognition from first level supervisors about the issues a ‘macho EMS culture’ fosters. He is passionate about eliminating the stigma attached to admitting a call has had an adverse effect and talks to agencies, regardless of their size about setting up peer support teams.
Daniel believes that there have been great improvements in equipment provision to better protect the health of the emergency responders, and yet many EMS agencies are slow to promote a culture of safety often due to the overall costs to do so. As someone who is in constant, at times, debilitating pain because there wasn’t the right equipment available when he was a field EMT simply due to such equipment had not been designed/built and emergency responder wellness, especially physical wellness didn’t have the focus it does now. He is an enthusiastic advocate for safe lifting, regularly speaking at conferences across the US.
How I Learnt To Live With Chronic Back Pain

Here at Mangar Health, we’re passionate about finding solutions to enable independence for people of all ages.
We’ve been talking to Hayley about her chronic illness and how a young person feels when pain prevents her living life to the full…
Chronic illness and chronic pain are expressions that I had seen used frequently online, but I didn’t really think that they applied to me. I’m 27 years old, I’m relatively fit and healthy, I don’t really get any sickness bugs or viruses and I only get a couple of colds a year. Despite all of the above, I have now been living with chronic pain for over 7 years.
I was 20 years old and in my first year of university when my back started hurting. One morning I woke up and was in complete agony, it hurt to move, it hurt to sit and it hurt to walk – it was completely debilitating. I booked a doctor’s appointment after putting up with the pain for a couple of days as it was showing no sign of getting any better.
I explained to the first doctor that I had fallen over two years previously and landed on my bum and as a result had had a sore back for a few days. I hadn’t experienced pain for years, but as it was in the same place I was a little concerned. The doctor had a look at my back and told me that I have scoliosis and that one of my vertebrae was pressing against the sciatic nerve which is what was causing the pain.
I was given a prescription for Diclofenac and Co-Codamol (8/500mg) in hopes it would help ease the pain. When the pain didn’t get any better, I returned to the doctors and was given a prescription for Naproxen and my Co-Codamol was increased to a higher dose (30/500mg).
At that stage, I was also referred to physiotherapy which took place in the hospital gym. There was a group of around 8 of us and I was the only one under the age of 50. The physiotherapy lasted for 6 weeks, which helped, but it didn’t stop the pain completely so I asked about having an X-Ray to see if there was an underlying issue that had not be found yet. I was told that as I was young and female, an X-Ray would be a really bad idea because it can be damaging for the reproductive organs.
Further down the line, I went to see a chiropractor who told me that I had the’ flattest feet she had ever seen’ and she advised that I be referred to a podiatrist to get orthotics to help my back in the long run. Apart from the referral to the podiatrist, the chiropractor didn’t help any more help with my back.
Since then I have been back to my doctor because I was in so much pain and my painkillers just weren’t strong enough. Once, I even ended up going to Minor Injuries at my local hospital because I had pain in my buttock and couldn’t walk or sit down. I’d never felt pain like it and was in absolute agony – at the hospital, I was told it was sciatica and advised to keep taking my painkillers. I also used a lot of heat patches over the next week or so which helped to ease the pain.
Towards the end of last year, I decided that I’d had enough of taking painkillers all the time and it was time I got some answers. I booked an appointment at my usual medical centre, but instead, I went to a different doctor – one that I had seen before about a different issue and I remember her being really helpful.
As soon as I explained everything, this new doctor was surprised that I had been taking such a strong dose of painkillers for so long, so she immediately referred me for an MRI scan to see what the problem is. I had my MRI scan in December and then I was referred to a surgeon who I saw in mid-March. It turns out the problem is not, in fact, my curved spine, but a prolapsed disc.
The surgeon couldn’t tell me exactly when the injury had occurred but he said that it sounded like it had been around seven years ago when I first started experiencing the pain. If it had been diagnosed at the time, I may have been able to have a simple surgery to fix it, but the disc has healed itself but in a way that is still causing me pain and there isn’t a lot that can be done for it now.
I’ve now been referred to a pain clinic at Derby Hospital so that they can assess my condition and find a new drug that won’t be as damaging to my organs as the Co-Codamol. I will also be going to regular physiotherapy sessions, but that’s not going to get rid of the pain completely.
My advice is – if there’s something wrong with you, trust your instinct. Doctors treat thousands of patients a day, so if your GP doesn’t refer you for further tests, don’t give up.
If you’re unsure on the advice you have been given it’s always worth asking for a second opinion.
Chronic pain and chronic illnesses are a nightmare, but there are options out there to help you. Luckily, I’m now getting the help I need since I asked for a scan and have seen the surgeon. My appointment for the pain clinic has now come through and I’m excited to get this sorted.
If you are living with a chronic illness, make sure you get advice from the appropriate healthcare professional and get access to assistive technology which might support you to live a full and happy life.
About Hayley Warren
 Hayley Warren is a 27-year-old Lifestyle Blogger from Birmingham. She is an Archaeology graduate from the University of Winchester, currently working as a full-time blogger and freelancer. She has been living with chronic pain for around 7 years.
Hayley Warren is a 27-year-old Lifestyle Blogger from Birmingham. She is an Archaeology graduate from the University of Winchester, currently working as a full-time blogger and freelancer. She has been living with chronic pain for around 7 years.
Twitter: https://twitter.com/xhjw
Blog: http://strangenessandcharm.co.uk/
Training at University Hospital of Wales, Cardiff

At the end of last year, one of our Sales Administrators, Rena, visited Cardiff University Hospital of Wales with Area Representative, John Finister. The internal sales team had been given the opportunity for one of them to attend a two-day student demonstration, so Rena jumped at the chance to experience a training session first hand.
As University Hospital of Wales is one of the top three schools in the UK for Occupational Therapists, Mangar Health organise a yearly demonstration of our key products to help raise awareness with students in their second year of study.
The students that take part in the training session have already carried out several placements in care homes and hospitals so they have a good understanding of the situations in which Mangar products could be used. With that in mind, the purpose of the demonstration and training was to show the value our products can have in those instances.
With over 70 students taking part the training events were split across two days and into two different 90 minute long sessions on each day – one on safe patient lifting and another on our bathing and bedroom products.
Bedroom and Bathing Training Sessions
The first session was made up of the Leglifter, Bathing Cushion and Archimedes, where John and Rena split the group in half. Rena lead the bathing half of the session, showing the students that everyday tasks such as bathing needn’t be difficult when you start to lose your mobility. At the same time John lead the bedroom session on the Leglifter. Although the Sit-U-Up and Handy Pillowlift were not on display the students were also given a brief introduction to them in this session.
Rena pointed out that “the students in my session were able to try the products out for themselves and although they were worried about sitting on the bathing cushion at first, they were amazed at the support it was able to provide to someone that may not be able to get into the bath themselves. Seeing the live reactions as they were using the bathing cushion was incredible and I felt proud that I was showing the future generation of OTs some life changing equipment that can really make a difference to someone’s life, whether they remain in their own home or go into care.”
Safe Patient Lifting Training Sessions
After the first session the two groups joined together for a presentation on the Camel and ELK lifting cushions, followed by the chance try them out themselves.
Rena said that “although they were apprehensive and a little nervous to lie on the floor, the end result was almost disbelief that they were able to be picked up at the touch of a button. It was great to be able to see the moment on their face where they realised the true value of the lifting cushions.”
“I really enjoyed the whole experience as I was able to benefit from talking to our future OTs. We found out what interested them about Occupational Therapy and why they wanted a career in it, which was really interesting when everyone had a different answer. “
“It was a pleasure working with John on these sessions and I went back to the office and urged everyone to take part so they could see people’s reactions first-hand. The students were receptive and chatty, which made the whole experience worthwhile for me.”
If you would like more information about our Product Awareness Events or training sessions please get in touch with the Mangar Health sales team (sales@mangar.co.uk).
Mangar ELK Lets Charlotte Play With Her 15-Week Old Baby

Charlotte has compartment syndrome and cellulitis which affects her legs and feet. She also has epilepsy which is tablet controlled. Her physical conditions affect her lower limb ability and she is unable to get down on the floor and back up again. As a result of this, Charlotte is unable to complete the exercises advised by the health visitor for her 15-week old baby. To carry out the exercises, her husband has temporarily given up work but is looking to return as soon as possible.
The Mangar ELK Lifting Cushion has enabled Charlotte to get down onto the floor and back up again, attend to her baby and encourage physical development in line with the expected stages for her child. Charlotte has been able to carry out the caring responsibility she has for her baby whilst maintaining her family relationship and support the development needs of her baby.
Safe Lifting
Her husband is now able to return to work and the baby is able to continue normal development. On occasions, Charlotte has also fallen due to her legs giving way. The Mangar ELK is a useful piece of equipment for her family to assist her to get up from the floor. Provision of this equipment has helped Charlotte maintain her independence and prevented calls to any care services.
Charlotte describes the impact of the lifting cushion in her own words “It’s been brilliant, it’s little things like being able to sort his clothes out in his room and also I’m happy that on Christmas day I’ll be able to sit on the floor and open his presents with him.”
Living With MS Made Easier With A Mangar ELK

Jennifer Humphrey, Plymouth
Jennifer Humphrey is 73 and lives in an assisted living apartment on the outskirts of Plymouth. A retired accounts administrator, she is treasurer of the residents’ social club and enjoys spending time with her 8 year old granddaughter Daisy.
Jennifer was diagnosed with Multiple Sclerosis in her early 50s after experiencing bowel and bladder symptoms often associated with the disease. She had also begun to notice dysfunction in one of her legs and doctors confirmed her condition as secondary progressive MS.
The problem – falls
After diagnosis, Jennifer learnt that her MS had caused degeneration of the seath around her nerves, this was causing loss information from her brain to her lower limbs, resulting in reduced mobility, her core strength remained good and she was able to continue working at her local Hospital with the assistance of a walking stick.
When her mobility first became more difficult, Jennifer’s husband was on hand to help, however he sadly died leaving Jennifer to manage her own needs. As time went on Jennifer mobility reduced significantly and she started to fall, as the number of falls increased, Jennifer found that she was increasingly unable to get herself up from the floor without help and became increasingly reliant on carers and ambulance services for support, which impacted her independence.
The experience of being lifted by carers was distressing and undignifying for Jennifer, she became concerned about the damaging effects this was having on her physical and mental health and to her care team as the task of lifting her was putting them at risk of a musculosketal injury.
Jennifer’s main goal was to find a way that she could be safely assisted up from the floor following a fall with minimal risk to herself and her carers.
The Solution – Mangar Elk
With the help from an Occupational Therapist and Mangar representative, Jennifer was recommended and provided with a Mangar ELK lifting cushion. This could be used by carers in her assisted living apartment, enabling them to support her to get up off the floor without needing to call for an ambulance. This was Jennifer’s first experience of Mangar products.
Jennifer said, “I’m not hurt when I fall but can’t get back up by myself. I feel very safe and secure when lifted on the ELK, it’s a very comfortable way to be lifted back up.”
The Mangar ELK lifting cushion enabled Jennifer to be assisted up from the floor in a safe and dignify way, it promoted best manual handling practise, helping to protect carers from musculoskeletal injury and reduced the need to call for ambulance crew support meeting all her goals.
Case Study: How A Complaint Led To A Better Lifting Solution

Since moving more than 15 years ago, Kevin’s remit has included policy development, risk management, accident investigation, training strategies and equipment guidance. A crucial part of the training strategy is to ensure all new staff joining undertake a manual handling course as part of their induction, with anyone who will be handling patients more required to attend an additional day of instruction.
During the second day of the course, staff are introduced to manual handling equipment including the Mangar Camel lifting cushion. The introduction of the Camel into the hospital’s manual handling equipment portfolio was triggered by a customer complaint 9 years ago.
Kevin says,
“We received a complaint from a member of the public that an elderly relative had fallen in the hospital during visiting time. They had asked staff for help to get up and been lifted using a hoist.
This had caused the elderly visitor some distress. They felt a hoist was undignified and shouldn’t be used on ‘non-patients’.
I had come across the Mangar Camel before and recognised that for uninjured people who have fallen, an inflatable lifting cushion provides a comfortable, dignified lift while still protecting staff from injury.
I recommended the introduction of Camels into our hospitals. We now keep the lifting cushions stored centrally and easily accessible on medical wards.”
Kevin believes there is still a culture among healthcare professionals of wanting to help a fallen patient before considering the risk of damage to themselves. HSE report that moving and handling injuries account for 40% of work-related sickness absence in health and social care and Kevin and his colleagues are committed to building awareness about the impact of musculoskeletal injury.
The training team hold regular manual handling drop-in training sessions and refresher courses to enable staff to develop their skills. Kevin concludes,
“We want staff to have the confidence to take a moment to assess a situation fully before deciding on the right way to move someone. We have to make sure we are protecting the long term health of our staff as well as ensuring our patients are moved safely.”
For more information on Mangar patient lifting devices, click here.
Steph Explains How The Mangar Bathing Cushion Makes Her Feel Normal Again

Mangar Customer, Steph, suffers pain in her knees caused by Osteoarthritis. This case study, written by OT Kate Sheehan, identifies how arthritis affects Steph’s everyday life and how using the bathing cushion allows her to bathe and feel ‘normal’ again.
Steph is 51, lives with her partner, she works full time in an accounts office for a local manufacturing company, and she adores her job as it gives her purpose, confidence and enjoyment.
Following suffering pain in her knees for a number of years she was diagnosed with Osteoarthritis in 2013 and had a subsequent diagnosis of Rheumatoid arthritis in September 2014, this has result in significant pain on mobility, reduced range of movement and joint stiffness, especially first thing in the mornings. Steph stated she has limited strength in her joints, including her knees and upper limb.
Steph is adamant she wants to continue to live a fulfilling life by managing her medical conditions, to enable her to continue to work, have a fulfilling leisure time and to maintain her dignity, her specific goals are,
- To independently access her bath, so she can soak her joints to reduce her pain and stiffness which improves her general mobility
- To reduce her anxiety and fear of being stuck in the bath
In addition to the client goals the OT intervention needed to meet the long-term needs of,
- Joint protection
- Fatigue management
- Client dignity and well-being
Environment
Steph’s lives in a privately rented bungalow, she has lived there for the last four years and hopes to stay as long as they can as they are settled in the area and have a number of close friends locally.
There is one bathroom, it comprises of a standard acrylic bath (1700mm by 700mm), close coupled toilet, shower cubicle and a pedestal wash hand basin. There is ample circulation space and clear access to the bath.
The bungalow meets Steph’s needs now and into the future, due to its off road parking, ease of access to the property, wide hallways and good-sized rooms throughout.
Task – bathing
Steph has difficulties with a number of activities of daily living, in particular bathing; she had stopped using her bath following an occasion when she became stuck in the bath for a number of hours, which caused her a huge amount of stress and anxiety.
Steph stated she had not bathed for nearly two years her decision was based on never wanting to be in a position whereby a complete stranger (firemen) maybe called upon to assist her to get out of the bath as her partners own health would preclude him helping.
Her particular areas of difficulty are,
- Lifting her legs over the bath if not in a seated position and free to use her arms to assist.
- Difficulty getting down to the bottom of the bath and back up again.
- Fatigue on carrying out the task
- Pain on carrying out the activity
Options
On reviewing the options to resolve the problem involved in the task, Steph took the opportunity to look at fixed bathlifts, reclining bathlifts and band bath lifts.
Fixed bath lifts – unsuitable as Steph nor her partner are able to lift the equipment in and out of the bath and Stephs partner did not want to use it. The fixed backrest did not enable Steph to soak all her joints to gain the maximum benefit of soaking in warm water.
Reclining bathlift – the same problems still existed as stated above. In addition although Steph was able to recline, this could not be achieved fully and to accommodate the lift her knees were flexed and not soaking in the warm bath water.
Band bathlifts – The band required good core strength/balance and Steph needed to shuffle into position, which caused pressure on Steph’s joints and pain on carrying out the activity
Steph trialed the Mangar Bathing Cushion, this allowed her to get right to the bottom of the bath, lie back and soak all her joints, thus achieving both Steph and the therapist’s goals.
Clinical reasoning
To be able to bathe allows us to maintain our personal hygiene, which is essential to our physical health and our mental well being. Steph needed to access to enable her to wash but also soak her joints to reduce pain and stiffness
The Bathing Cushion has give Steph the confidence to bathe independently and in her own words
‘Return to doing something that I have been deprived of for a number of years and to do something that is normal which makes me feel normal’
This case study is written using the PET occupational therapy model. In 1996 Law et al developed the person environment occupation model as a response to an identified need of occupational therapy, which describes the theory and application of the interaction between the person (P), their environment (E) and the task (T) or occupation. The model gives a defined framework to enable OT’s to concisely clinically reason their intervention.